











The coffin bone, also known as the distal phalanx or P3, is located at the tip of the horse’s limb inside the hoof capsule. It is suspended within the hoof by laminar tissues and surrounded by soft tissue structures, with the hard hoof wall forming its external protection.
Its unique shape provides the foundation for weight-bearing and shock absorption with every stride. Although hidden from view, this bone plays a pivotal role in supporting the horse’s entire body and transferring forces through the hoof capsule.
When the supporting structures or blood supply around the coffin bone are disrupted, various lameness issues can occur. In cases of founder, the most advanced form of laminitis, the coffin bone rotates or sinks, causing acute pain. Chronic stress or concussion can lead to pedal osteitis, a degeneration of the bone surface, while direct trauma or excessive loading may result in fractures.
Early detection of coffin-bone–related lameness is key to preserving soundness. You can use hoof testers to pinpoint areas of tenderness, monitor digital pulse and heat changes at the coronary band, and work with your veterinarian to identify rotation, sinking, or bone erosion.
Read on to learn more about the coffin bone, related forms of lameness, and how to detect them so you are prepared if one of your horses seems unsound.
Coffin Bone Anatomy in Horses
The Distal Interphalangeal (DIP) joint in the horse’s hoof is a complex structure formed by three bones: [1]
- Distal sesamoid or navicular bone
- Short pastern, or P2 bone
- Coffin bone
The coffin bone is also referred to as the pedal bone, P3, and the distal phalanx. It sits lowest to the ground within the hoof capsule. [1]
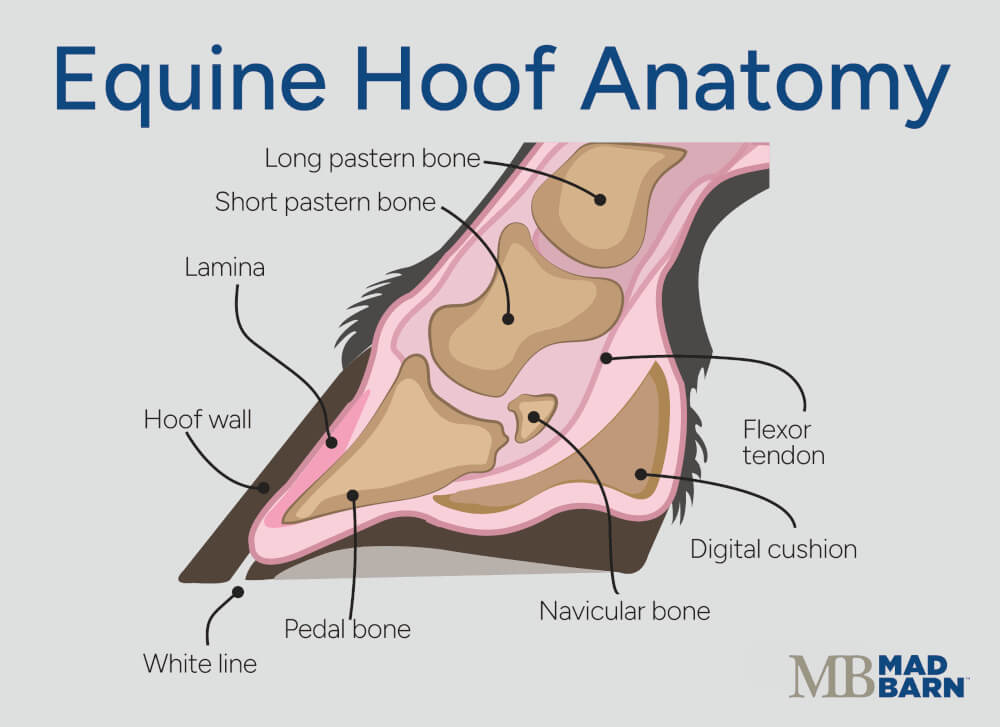 Illustration: Dr. Ana Mesa, PhD
Illustration: Dr. Ana Mesa, PhD
The coffin bone gets its name because it is fully enclosed within the hoof capsule, much like a body encased in a coffin. This wedge-shaped bone attaches to the hoof wall through laminar tissue and plays a key role in weight-bearing and shock absorption. [1]
The surface of the coffin bone is irregular, with a thin, curved solar margin along the bottom and rounded palmar (rear) processes. Numerous small vascular openings (foramina) across its surface allow blood vessels to pass through, supplying the bone and the surrounding sensitive tissues. [1]
5 Types of Coffin Bone Lameness
Because of its location within the hoof, the coffin bone is prone to trauma and is associated with several different types of lameness in horses.
These conditions range from acute fractures to chronic degenerative changes from repeated concussion, each involving different types of damage to the coffin bone.
Contributing factors such as abnormal hoof conformation, improper farriery, and hard footing can increase stress on the coffin bone and influence the severity of lameness.
Here are the top five most common types of coffin bone lameness in horses.
1) Ringbone
Low ringbone refers to osteoarthritis of the distal interphalangeal (DIP) joint, also called the coffin joint. This degenerative condition develops when cartilage within the joint breaks down, leading to inflammation, new bone growth, and joint stiffness.
It is more common in the forelimbs than the hind limbs and can cause mild to severe lameness depending on the extent of joint damage. [2]
Other signs of low ringbone may include hard swelling or thickening around the coronary band and, in some cases, joint effusion (fluid buildup within the coffin joint). [2]
Diagnosis & Treatment
Veterinarians can diagnose lameness caused by low ringbone using nerve blocks to localize the source of pain. [2] Additional diagnostic methods for confirming low ringbone may include: [2]
- Radiography (X-rays)
- Ultrasound
- Nuclear scintigraphy (bone scan)
- Computed tomography (CT scan)
- Magnetic resonance imaging (MRI)
- Arthroscopy (exploratory surgery)
Low ringbone cannot be cured but is usually managed using a combination of methods, including: [2]
- Non-steroidal anti-inflammatories (NSAIDs)
- Chondroprotectant medications
- Intra-articular corticosteroid injections
- Hyaluronic acid (HA) injections
- Stem cell therapy
- Autologous protein injection (Prostride®)
- Shockwave therapy
- Shoeing modifications
The prognosis for low ringbone is guarded to fair, depending on the severity of the individual case. [2]
What's your top priority with your horse's health?
Enter your email to receive your store credit
2) Fractures
Fractures of the coffin bone are another common cause of lameness. They are usually caused by direct trauma to the hoof. [3][4] These fractures can vary in severity, ranging from small stress fractures to more significant breaks that affect joint stability and hoof function.
Lameness from coffin bone fractures is often more noticeable when the horse is turning. Other signs of a coffin bone fracture may include: [4]
- Heat in the foot
- Increased digital pulse
- Sensitivity to hoof testers
Fractures of the coffin bone can occur in any horse but are most common in racehorses due to the high impact and stress placed on their hooves. Recovery can be challenging, and many affected horses never return to their previous level of performance. One study reported a 50 to 63% success rate for returning to racing after a coffin bone fracture. [3][5]
Fractures of the coffin bone usually occur in the fore limbs but can occasionally affect the hind limbs as well. They are classified into seven different types based on their location and prognosis. [5]
Type I
Type I fractures involve the “wings” of the coffin bone, which are the thin, flat extensions on either side of the bone that help anchor soft tissues within the hoof. Because these fractures occur in the wings and do not extend into the DIP joint space, they are often referred to as “wing fractures.” [4][5]
Clinical signs may include localized sensitivity when using hoof testers and an increased digital pulse on only one side of the hoof. [4][5]
A unilateral palmar digital nerve block can help localize the pain, but X-rays are the primary diagnostic tool. Standard views may not always reveal the fracture, so angled views are often required. [4]
Type I fractures generally heal within four to six months, although the fracture line may remain visible on X-rays for longer. The prognosis for returning to athletic use is considered fair to good. [4]
Type II
Type II fractures are vertical articular fractures that extend into the DIP (coffin) joint. They can be difficult to distinguish from Type I fractures based solely on clinical signs, as both cause localized lameness, but Type II fractures typically result in more severe lameness and visible joint effusion. [4]
Because of the domed shape of the coffin bone, a Type II fracture may appear as two fracture lines on X-ray, one at the top and one at the bottom. This can sometimes be mistaken for multiple separate fractures or a comminuted fracture, where the bone is broken into several pieces. [4]
The prognosis for Type II fractures is generally worse than for Type I due to the risk of osteoarthritis developing in the DIP joint. However, the outlook is still considered fair to good, and it is more favorable than for Type III fractures.
Younger horses (under three years old) tend to heal better and have a more positive long-term prognosis compared to older horses with this type of fracture. [4]
Type III
Type III fractures are distinct as they bisect the coffin bone into equal halves. [4][5] The signs and diagnostic methods for Type III fractures are the same as for Type II fractures. [4][5]
Type III fractures can be treated medically or surgically. Medical treatment carries a good prognosis for return to ridden exercise in horses younger than three years of age and a more guarded prognosis in older horses.
Surgical treatment of Type III fractures results in a fair prognosis if no complications arise. [4]
Type IV
Type IV fractures involve the extensor process of the coffin bone, a bony projection serving as the insertion point for the long digital extensor tendon. These fractures can be caused by hyperextension injury, avulsion injury, or developmental disorders of the bones and cartilage. [4]
In some horses with a Type IV fracture, bone fragments may not cause symptoms and are only found incidentally on X-rays. In other cases, clinical signs of a Type IV fracture may be similar to those seen with other conditions of the DIP joint, with joint effusion and lameness isolated to the DIP joint or foot. [4]
Surgical treatment of Type IV fractures appears to carry a good short-term prognosis. However, one study showed less than half of horses remained sound four years after surgery. Even with surgery, the DIP joint may require long-term medical intervention to manage pain. [4]
Type V
Type V fractures involve multiple fractures of the coffin bone and result in severe lameness. They usually involve the DIP joint and cause effusion. [4]
Type V fractures usually occur from trauma to the foot. They can also occur secondary to septic osteitis, a bacterial infection of the foot, or sequestra (piece of dead bone separated from healthy bone). Other types of coffin bone fractures can progress to a Type V fracture if further trauma is sustained. [4]
Type V fractures may be mistaken for other types of fractures on initial X-rays, and additional views or special techniques may be required to ensure accurate diagnosis. If infection occurs, local surgical debridement is needed, but otherwise, surgical treatment is not used for Type V fractures. [4]
Type V fractures have the poorest prognosis of all coffin bone fracture types. This is due to the presence of multiple fragments, the instability of the fracture, and joint involvement. However, it is sometimes possible to manage a Type V fracture well enough to maintain quality of life for in-service broodmares or pasture pets. [4]
Type VI
Type VI fractures are fractures along the solar margin. They occur in mature horses and usually cause mild lameness. They may also be identified incidentally on X-rays of sound horses. Type VI fractures occur mainly in the forelimbs and usually occur between the quarters and the toe, toward the front of the foot. They are often seen in horses with thin soles and other signs of coffin bone inflammation. [4]
Type VI fractures can be caused by trauma or occur secondary to laminitis or other types of hoof disease. Horses working on hard surfaces may be predisposed to this type of fracture as well. [4]
In the acute stages, horses may show sensitivity to hoof testers, though this is not always the case. They may also present with a history of general “foot soreness.” The lameness responds to either a palmar digital or abaxial sesamoid nerve blocking. [4]
Type VI fractures may involve multiple fragments or only one. Most fragments heal by resorption or form a fibrous union if horses are given extended rest. [4]
The prognosis for Type VI fractures is good if the horse is given a suitable rest period, but if other issues such as laminitis are involved, the prognosis depends on the specific pathology. [4]
Type VII
Type VII fractures are similar to Type VI but are specific to foals. They occur in a consistent location at the junction of the palmar/plantar process and the body of the coffin bone. [4]
Type VII fractures appear to be common. In fact, 74% of foals in one study group were found to have one or more coffin bone fractures. The average age for fracture occurrence was three to four months. [6]
Unlike Type I fractures, which occur on the palmar/plantar process, Type VII fractures begin and end at the solar margin. They are thought to be caused by excessive force on the deep digital flexor tendon or coffin bone during weight-bearing. [4]
Type VII fractures may be associated with low-grade lameness, but in some instances, there may be no lameness at all. Unlike other types of coffin bone fractures, clinical signs of Type VII fractures may resolve on their own before radiographs are taken. [4][6]
If a Type VII fracture is diagnosed, treatment involves exercise restriction. Corrective farriery is not usually necessary. The long-term prognosis is excellent. [4][6]

Treating Coffin Bone Fractures
There are both surgical and non-surgical treatment options for most types of coffin bone fractures. Surgery is mainly used when the DIP joint is involved. If a penetrating injury was the cause of the fracture, that needs to be treated as well. [4]
Nonsurgical treatment options typically include: [4]
- Remedial farriery
- Foot casts
- Stall rest
- Controlled exercise
- Administration of NSAIDs
These methods are also used to aid recovery after surgical treatment. [4]
Remedial Farriery
Remedial farriery helps create complete immobilization of the foot by restricting the heels from expanding. It typically involves a foot cast, rim shoe, or bar shoe with multiple clips. [4]
Foot casts are usually placed around the entire foot, including the coronary band. Since casting material is highly restrictive, foot casts that enclose the coronary band require close monitoring to prevent complications. [4]
More recently, casting material made with ballistic grade polyester has been introduced, which allows a cuff to encase the foot while staying below the coronary band. This type of cast is associated with fewer complications. [4]
For Type III fractures, intra-articular treatment of the DIP joint for synovitis or osteoarthritis may also be recommended. [4]
Surgery
Surgical treatment of coffin bone fractures often involves removing bone fragments and/or repairing the coffin bone with screws. Potential complications include: [4]
- Increased risk of infection,
- Failed repair of the fracture
- Impingement of the screws on adjacent structures
- Osteoarthritis of the DIP joint
Surgical treatment has a higher rate of complications and is more expensive than non-surgical options. On the other hand, successful surgery provides the most reliable long-term repair of the DIP joint. [4]
With many coffin bone fractures, ongoing monitoring with periodic X-ray is recommended to assess healing. When treatment protocols are followed, lameness usually decreases over the first two to four weeks. Most horses are sound at the walk within four to eight weeks. [4]
For horses with chronic lameness, neurectomy is a last-resort option. This procedure desensitizes the foot but does not stop any degenerative conditions. [4] Horses with neurectomies are not permitted in competition, and many veterinarians no longer recommend this procedure.
3) Subchondral Cysts
Subchondral bone cysts, also called subchondral cystic lesions (SCLs) or osseous cyst-like lesions (OCLLs), are the most common cyst-like lesions seen in horses.
However, they are not true cysts because they lack an epithelial lining and often communicate with the joint. They tend to develop in horses between three and 18 months of age. [7][8]
Subchondral cysts can occur in multiple bones, with the DIP joint being the second-most common location after the femoral condyle. They usually involve the subchondral bone and can vary in size or shape. They may be deep or shallow. [7]
Risk factors for subchondral cysts in horses include: [7][9]
- Genetic predisposition
- Inadequate nutrition
- Abnormal growth rate
- Hormonal imbalances
- Existing osteochondritis
- Biomechanical issues
- Injuries
Subchondral cysts of the coffin bone are more frequently diagnosed in male horses. Thoroughbreds also appear to be affected more often than other breeds. These cysts may occur in either the fore limbs or hind limbs. [7]
Most cysts affecting the coffin bone occur near the center of the bone. Clinical signs may include: [7]
- Effusion (fluid accumulation) around the DIP joint
- Effusion around the fetlock joints
- Lameness
Diagnosis
Subchondral cysts are usually diagnosed using nerve blocks and X-ray. [7]
Radiographic characteristics of these cysts depend on their stage of development. They may appear as: [7]
- A small flattening or depression in the articular surface
- Circular or oval-shaped dark spots within the bone
CT and MRI may also be helpful in diagnosing subchondral cysts. [7]
Treatment
Treatment may be conservative, with controlled exercise and symptomatic use of NSAIDs, or it may be surgical. Conservative treatment of coffin bone cysts appears to have a poor success rate. [7]
Surgical treatment aims to prevent enlargement of the cyst and promote filling of the lesion with osseous material. Surgical debridement, where dead or damaged bone tissue is removed, appears to have the highest success rate (70 – 90%). [7]
More recently, arthroscopic intra-articular steroid administration directly within the cysts has been recommended. This approach is reported to have an improved success rate and shorter recovery time. [7]
The prognosis for return to performance for horses with subchondral cysts of the coffin bone varies widely from 30 to 90%. Prognosis depends on the breed, age, use of horse, surface area of affected cartilage, concurrent osteoarthritis, and type of treatment. [7]
4) Collateral Ligament Injuries
The collateral ligaments of the DIP joint are located deep within the hoof capsule. They support the DIP joint in various types of movement. [10]
In sport horses, desmopathy of the collateral ligaments of the DIP joint (CL-DIPJ) is a common cause of lameness. In fact, these ligaments are the most affected structures in the hoof region. Horses aged nine or older are at higher risk for this disorder. [10][11]
CL-DIPJ injury is believed to result from biomechanical stress caused by rotational forces in the coffin bone as the hoof strikes the ground. Chronic medial-lateral hoof imbalance appears to be a contributing factor. Angular hoof deformities may also predispose a horse to CL-DIPJ disease. [11]
Equestrian sports that involve circular movements in conjunction with sudden stops (e.g. reining) or exercise on uneven ground may also contribute to CL-DIPJ injury. [11]
Horses with CL-DIPJ desmopathy may not have specific clinical signs, but they usually have acute or chronic lameness that can vary in severity. The presentation of lameness may change with the direction of movement and footing. [10]
Diagnosis & Treatment
MRI is considered the gold standard for diagnosing CL-DIPJ in horses. [10] X-rays and ultrasound may also be helpful in some cases. The condition is sometimes diagnosed by analgesia of the palmar digital nerve blocks or intra-articular anesthesia of the DIP joint. [10]
Treatment involves rest and remedial farriery. In some cases, injections of therapeutic biologics or extracorporeal shock-wave therapy can also aid healing. The prognosis for return to athletic use is good. [10]
5) Sidebone
Sidebone in horses describes cases where cartilage in the hoof turns into bone (ossifies). It is likely caused by concussive forces on the hoof.
Sidebone is most common in the fore limbs of heavy horses or those with conformational abnormalities. [12] [13]
The cartilages of the horse’s hoof serve three main purposes: [12]
- Provide support to the bottom aspect of the foot
- Dissipate forces incurred when the foot makes impact with the ground
- Aid in blood return from the limb
When the cartilages ossify, their ability to dissipate force is reduced. Extensive ossification reduces the hoof’s flexibility. These changes result in forces being transferred to other structures in the foot, which can lead to adaptive changes or injury in other tissues. [12]
In horses with sidebone, ossification typically begins at the base of the collateral cartilage and progresses inward. In some cases, it may also develop from a separate center of ossification. The lateral (outer) side of the hoof is more commonly affected than the medial (inner) side. [12][13]
Treatment & Prognosis
The severity of ossification in sidebone can be measured using a grading system from 0 to 5, with 0 indicating no ossification and 5 representing the most severe changes:
- 0: No visible ossification (normal cartilage)
- 1–2: Mild ossification with small mineralized areas
- 3: Moderate ossification with larger or more distinct mineralized regions
- 4–5: Severe ossification with extensive mineralization and possible fusion to surrounding bone
Because of the close anatomical relationship between the foot’s collateral cartilages and the collateral ligaments of the DIP joint, sidebone is sometimes associated with collateral ligament injuries. [12]
Sidebone is rarely the primary source of lameness, though horses with this condition may have a shortened stride. Instead, it is usually an incidental finding during physical examination or X-rays of the feet. Extensive ossification can be palpated near the coronary band. [12][13]
In rare cases, ossified cartilage can fracture. Signs of a fracture include localized heat, swelling, and pain upon palpation. [13]
Sidebone cannot be reversed once the cartilage has ossified. Treatment is symptomatic and includes rest and NSAID medications. Any hoof imbalances should also be addressed. If lameness persists, unilateral neurectomy or surgical excision of ossified cartilage can be performed as a last resort. [13]
The prognosis is generally good for horses with sidebone unless lameness is severe enough to require surgery, in which case the outlook is more guarded. [13][14]
Preventing Coffin Bone Lameness in Horses
Regular hoof care and veterinary evaluations are key to preventing and detecting coffin bone lameness early. Schedule formal lameness exams at least once a year, or more often if your horse shows signs of discomfort.
Work with an experienced farrier to maintain proper hoof balance. Routine trims every 4–6 weeks, or shoeing when required, keep the hoof capsule aligned, distribute weight evenly, and reduce stress on the distal phalanx.
A well-planned training program also helps protect the coffin joint. Introduce new work gradually, alternate high-impact exercises with low-impact activities such as walking on varied terrain, and schedule rest days to allow hooves to recover. Maintaining an ideal body condition score is equally important, as excess weight increases the forces placed on the hoof.
Finally, good nutrition is essential for hoof strength and overall soundness. Provide a balanced, forage-based diet that supplies adequate vitamins, minerals, and protein to support hoof health and connective tissue strength. A complete vitamin and mineral supplement, such as Mad Barn’s Omneity, helps ensure your horse receives all the nutrients needed to build strong, resilient hooves.

If you are unsure whether your horse’s diet is meeting all their requirements, book a free nutrition consultation with one of our qualified equine nutritionists.
Frequently Asked Questions
Here are some frequently asked questions about coffin bone anatomy and lameness in horses:
The coffin bone, or distal phalanx (P3), is the lowermost bone in the horse's hoof capsule. It is part of the Distal Interphalangeal (DIP) joint and provides weight-bearing support and shock absorption with every stride.
The coffin bone endures constant concussion and shear while the horse is standing and walking. Disruptions in blood supply, improper hoof balance, hard footing, or trauma can lead to inflammation, degeneration, or fractures in the DIP joint.
The top five conditions affecting the coffin bone are: Low ringbone (osteoarthritis of the coffin joint), fractures of the distal phalanx, subchondral cysts, collateral ligament desmopathy, and sidebone (ossification of the collateral cartilages).
To prevent coffin bone issues in your horse, it's important to maintain balanced hoof trimming and appropriate shoeing, avoid prolonged work on hard surfaces, monitor for early signs of heat or digital pulse changes, and schedule regular veterinarian and farrier evaluations.
Summary
The coffin bone is the lowermost bone in the horse's limbs, making up part of the Distal Interphalangeal (DIP) joint. Its position as the main weight-bearing bone of the foot makes it a common source of lameness.
- The coffin bone is also known as P3, the pedal bone, and the distal phalanx
- Coffin bone conditions associated with lameness include low ringbone, fractures, subchondral cysts, collateral ligament injuries, and sidebone
- These conditions can lead to varying degrees of lameness and have differing treatment options
- Staying up-to-date with routine lameness exams and consistent farriery help prevent coffin bone lameness
References
- Dyce. K. M. et al., Textbook of Veterinary Anatomy. 4th ed. Saunders Elsevier, St. Louis, Mo. 2010.
- Moorman. V. J. and Beasley. B., Osteoarthritis of the Distal Interphalangeal (Coffin) Joint in Horses. Merck Veterinary Manual. 2024.
- Robson. K. E. et al., Palmar or Plantar Process Fractures of the Distal Phalanx in Riding Horses: 22 Cases (1994–2003). Equine Veterinary Education. Wiley. 2008.
- Kidd. J., Pedal Bone Fractures. Equine Veterinary Education. Wiley. 2011.
- Schade. S. M. et al., The Microvasculature in the Equine Distal Phalanx: Implications for Fracture Healing. Veterinary and Comparative Orthopaedics and Traumatology. Georg Thieme Verlag KG. 2014. View Summary
- Faramarzi. B. et al., Incidence of Palmar Process Fractures of the Distal Phalanx and Association with Front Hoof Conformation in Foals. Equine Veterinary Journal. Wiley. 2015. View Summary
- Sherlock. C. and Mair. T., Osseous Cyst-like Lesions/Subchondral Bone Cysts of the Phalanges: Phalangeal Osseous Cyst-like Lesions. Equine Veterinary Education. Wiley. 2011.
- Pérez-Nogués. M. et al., Treatments and Prognosis for Subchondral Cystic Lesions in the Distal Extremities in Thoroughbred Prospect Racehorses. Animals. MDPI AG. 2023. View Summary
- Jenner. F., Treatment of Osseous Cyst‐like Lesions. Equine Veterinary Education. Wiley. 2021.
- Moorman. V. J. and Beasley. B., Collateral Ligament Desmopathy of the Distal Interphalangeal Joint in Horses. Merck Veterinary Manual. 2024.
- Camargo. G. G. et al., Risk Factors for the Occurrence of Desmopathy of the Collateral Ligaments of the Distal Interphalangeal Joint in Equines – A Cross-Sectional Study. Acta Veterinaria. Walter de Gruyter GmbH. 2020.
- Dyson. S. et al., Is There an Association between Ossification of the Cartilages of the Foot and Collateral Desmopathy of the Distal Interphalangeal Joint or Distal Phalanx Injury?. Equine Veterinary Journal. Wiley. 2010.
- Moorman. V. J. and Beasley. B., Sidebone in Horses (Ossification of the Collateral Cartilages). Merck Veterinary Manual. 2024.
- Ross. M. W. and Dyson. S. J., Eds., Diagnosis and Management of Lameness in the Horse. 2nd ed. Elsevier/Saunders, St. Louis, Mo. 2011.























